
Silver Linings: Next-Gen Anti-Pandemic Tech and How to Protect Yourself Now
In December 2024 we discuss upcoming vaccine technology and explore the ongoing risk and potential effects of long COVID.

Written by J. A. Sterling and Adam Tsuris
SCORE’s seasonal update for December 2024 presents the latest findings related to the ongoing COVID-19 pandemic. Everything here is based on peer-reviewed science. Conclusions and recommendations apply the precautionary principle. You can find our previous Seasonal Update Summer 2024 here.
This time, publishing in December 2024, we present a positive forward outlook on upcoming vaccine technology, and we explore a major driver of continued COVID caution, the ongoing risk and potential effects of Long COVID.
Socialist COVID-19 Organizing, Resistance, and Education (SCORE) is the organization behind Dynamic Zero. Join us today! We always seek to support one another and to keep each other safe. We extend this warm solidarity to all our readers. Stay safe out there!
Pandemic Outlook
Next-Generation Vaccines
The development of new and promising vaccine technologies represents an opportunity to transform the trajectory of the COVID-19 pandemic, an opportunity unseen since 2020. The increasing number of potentially more effective vaccine candidates, many converging on a mucosal nanoparticle “prime-and-spike” strategy, brings hope for a future with fewer infections and reduced viral spread. While current vaccines have significantly reduced fatalities and severe acute presentation of illness, they have not established a sustainable path forward, leaving the virus unmanaged in the absence of widespread non-pharmaceutical interventions (NPIs).
SARS-CoV-2 may ultimately resemble measles—a virus that can be eradicated with universal, sustained vaccination—or it might prove more akin to tuberculosis, influenza, malaria, or HIV, requiring ongoing, multi-faceted strategies to mitigate its effects. Achieving sterilizing immunity—a state where vaccinated individuals neither get infected nor transmit the virus—remains the ideal goal, though other workable outcomes may be possible. If future vaccines achieve sterilizing immunity, the task becomes one of global coordination to universally administer these vaccines indefinitely, addressing not only human cases but also the challenge posed by animal reservoirs. Alternately, if SARS-CoV-2 cannot be eradicated, vaccines will remain a critical component of a broader public health strategy that includes NPIs, air cleaning, and surveillance testing to control transmission and reduce disease burden.
Understanding where COVID-19 falls on this spectrum is essential, as the stakes include not just the immediate reduction of suffering, but the prevention of long-term outcomes we do not yet fully understand. Vaccines that reduce transmission and disease burden could, when combined with strategies like air cleaning, targeted NPIs, and robust global solidarity, substantially lower the virus's impact. However, any vaccine-centric approach will require not only scientific breakthroughs but also universal and equitable administration, a challenge magnified by our political and economic system which prioritizes profit over human lives.
This brings us to one of the most promising advancements in vaccine development: targeting the virus at its primary entry point. By focusing on the nasal mucosa, next-generation vaccines aim to bolster the body's defenses where the virus first gains a foothold, potentially stopping infections before they spread further into the body.
Viral exposure in the nose via vaccines has long been an established technique to remotely help prepare the lungs to fight off severe infections, even without the virus directly reaching the lungs.1 Early exposure in the nose and upper airways can help the lungs respond more quickly and effectively to infections by activating both innate (non-specific) and adaptive (learned from exposure) immune defenses. The exact processes linking them are not fully understood.
Consequently, next generation nasal vaccine candidates aim to stop the virus at its entry point—the nasal mucosa. For instance, in the United States, the NIH is testing MPV/S-2P,2,3 a nasal spray vaccine designed to create strong immune defenses in the nasal passages, with the claim that infection and transmission may be prevented at their source. MPV/S-2P began Phase 1 trials in July 2024. Similarly, already in Phase 2, the CVXGA vaccine candidate is intranasally applied and uses a modified parainfluenza virus 5 (PIV5) vector to produce an immune response and potentially prevent transmission.4,5 PIV5 causes Kennel Cough in dogs.
Other mucosal vaccines are also showing promise, although trials have not yet begun. One uses a weakened version of SARS-CoV-2 to potentially provide protection.6 Another combines spike proteins from multiple virus variants with measles and mumps vaccine technology to protect against a wide range of strains while producing robust antibodies.7 A third employs a Newcastle Disease Virus to deliver the spike protein; while it is in phase 2B, data is unavailable supporting its claim to potentially prevent infection and transmission.8
Beyond this technology, vaccine designs utilizing novel nanoparticles, different from those used for the first generation of COVID-19 vaccines, offer increased stability and broader protection. The most promising candidate after MPV/S-2P is built on a stomach bug nanoparticle (H. pylori)9 and appears to confer protection through the current JN.1 descendants. Another candidate utilizes SARS-CoV-2 plasmid DNA, offering more stability and similar neutralization compared to mRNA while also cross-reactive against multiple variants.10 Another, mosaic-8b, includes components from multiple SARS-like viruses, preparing the immune system to combat emerging disease, not just COVID–19.11 These innovations aim to provide longer-lasting protection while significantly reducing and hopefully eventually eliminating or driving the risk of infection and transmission low enough to eradicate COVID-19.
Innovations that refine current-gen vaccines:12
- Vaxart is in Phase 2B evaluating an oral tablet vaccine against the efficacy of the currently approved COVID vaccines.13 If realized, an oral vaccine will vastly improve the ease of distribution, eliminating the need for vaccinators to be capable of administering intramuscular injections, reducing refrigeration requirements, and will reduce vaccine hesitancy in people who dislike needles.
- PopVax will shortly begin their trial of a new vaccine that will hopefully provide cross-reactive protection against current and future predicted COVID variants.14
- Iran’s Razi Cov Pars is in Phase 4 trials for a vaccine comparable to those currently available, but with an added intranasal dose after two injected doses to evaluate longer-lasting and broader protection.15
- The Phase 3 trial of CanSino’s Convidecia vaccine evaluated a comparison of injected dose vs inhaled through an asthma puffer and found the results comparable for both excepting significantly fewer side effects when inhaled.16
- The Patria vaccine developed by AviMex in Mexico available in both injected and intranasal forms passed through Phase 2 approval. It aims to add a lower cost vaccine for middle and lower income countries.17
- LUNAR-COV19 (trade name Kostaive), a samRNA vaccine, was recently approved in Japan as an ostensible durable and variant-proof vaccine. samRNA (“self-amplifying mRNA”) induces an antibody response at lower vaccine doses than mRNA, so it saves production costs and reduces side effects.18
- GEO-CM04S1 is in Phase 2 trials as a durable and variant-proof vaccine, with promising results for people with immunosuppression. It includes both Spike and Nuclear proteins (current generation vaccines only include the Spike protein or fragments thereof).19
- Note that in the bullets above, clinical trial phases may correspond to the originating country's approval system.
Taking all of this profit-motive-constrained innovation into account, CIDRAP released a 2028 roadmap which targets production of a broadly applicable, long-lasting vaccine with high activity in the mucosa of the upper and lower respiratory tracts thus potentially preventing transmission and infection.20
At present, each of these vaccines offers exciting potential to reshape how we manage the pandemic, targeting not just severe illness but also the virus’s ability to spread. While we await these advancements, staying up to date with current vaccines remains essential.
Next-Generation Antivirals
While it’s not on the market yet, an exciting new class of antivirals has recently been developed called viral methyltransferase inhibitors. As opposed to Paxlovid, which targets the tools a virus uses to replicate, this new antiviral targets the virus’s innate ability to replicate (within its RNA), providing a new tool in the body’s fight against COVID-19.
This new antiviral is expected to have minimal side effects, to be as effective as Paxlovid when taken on its own, and to be able to be used in conjunction with Paxlovid in order to fight COVID even more effectively. Like Paxlovid, it runs no more risk than any liver metabolized drug, and unlike antibiotics which can hurt the host as well as the infection, this technology is formulated to stop viral replication and does not target the host.
Additionally, it’s been shown to be effective even if COVID mutates in response to it, and is expected to be effective against a wide variety of viruses in addition to SARS-CoV-2. The world may soon have a new tool to use in fighting our ongoing pandemic and in fighting future pandemics as well.21 First though, a candidate drug molecule needs to make it out of the lab and into clinical trials.
Long COVID Prioritization
The rate of COVID–19 deaths are declining by even the most conservative metric, a phenomenon to be explored in a future Dynamic Zero article. Perhaps this is due to having socially murdered the most vulnerable, or the remaining most vulnerable having adapted their lifestyle (further invisibilized as a result); and, in parallel, perhaps due to the majority pre-disabled population obtaining some level of protection from a combination of infection and vaccination while medical techniques for preventing death have been improved and widely disseminated.
A COVID–19 infection is by definition severe, and certainly worse than the flu,22 whether or not the presenting symptoms are severe, externally invisible, and/or minimized by the patient or others; however, the risk to our future and our long-term survival is the long term impact of infection. A recent study by the National Academy of Sciences was completed, surveying (and summarizing) current official definitions of Long COVID, and the final official recommendation for definition (located here) and summarized in the following infographics.
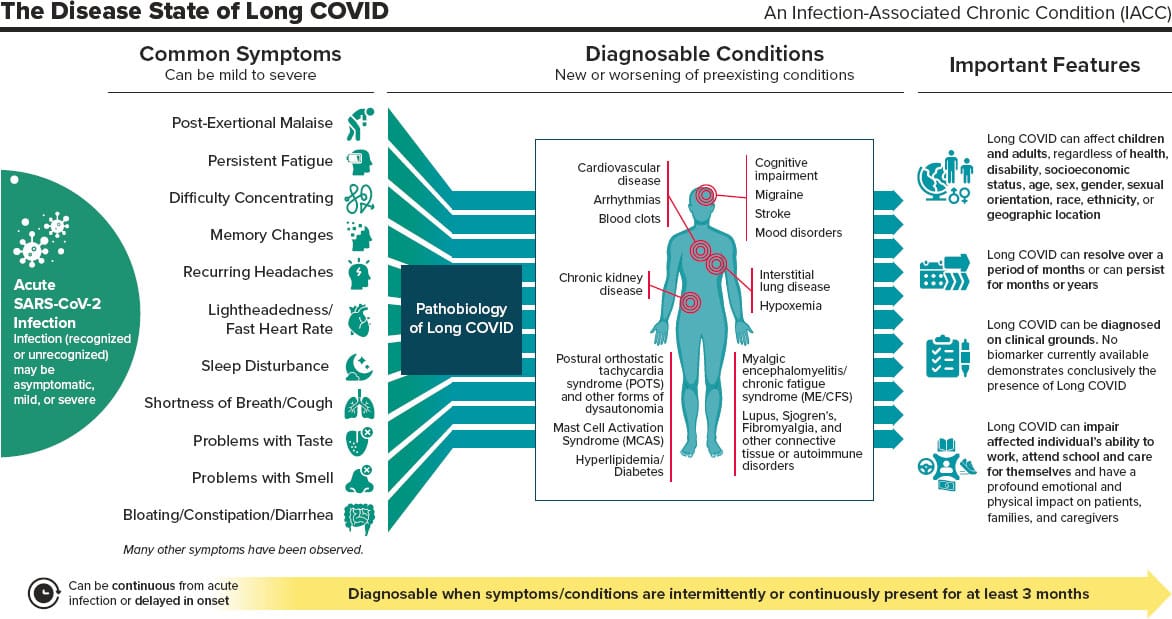
Many patients infected with SARS-CoV-2 only exhibit mild symptoms and 30%–60% of cases have none at all;23 however, regardless of acute infection severity and regardless of COVID variant, each infection risks long-term symptoms, and each reinfection increases that risk24—the damage is cumulative. According to the CDC25 and Moderna,26 the average risk of developing Long COVID is approximately 20% (1 in 5) and this risk only increases with each subsequent infection.27 The risk is the same for children,28 athletes, and everyone else.
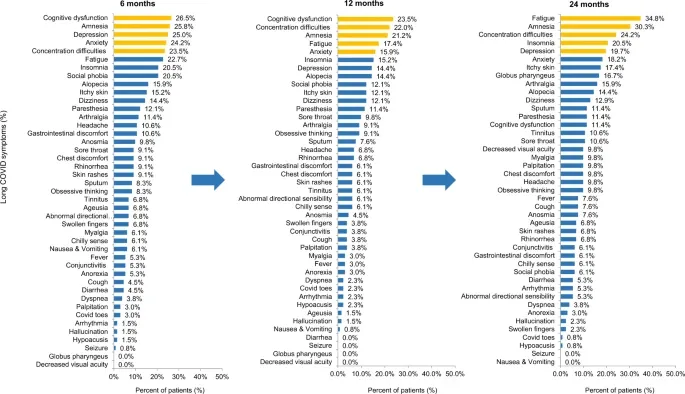
Long-term symptoms, their longevity, and their prevalence as experienced up to two years after a 2021 infection are summarized in the series of bar graphs and the table below.
| Time Post-Infection | Percentage Reporting Symptoms | Most Common Symptoms (%)29 |
|---|---|---|
| 6 months | 59.8% (79/132) | Cognitive dysfunction (26.5%), amnesia (25.8%), depression (25.0%), anxiety (24.2%), concentration difficulties (23.5%) |
| 12 months | 53.0% (70/132) | Cognitive dysfunction (23.5%), concentration difficulties (22.0%), amnesia (21.2%), fatigue (17.4%), anxiety (15.9%) |
| 24 months | 71.2% (94/132) | Fatigue (34.8%), amnesia (30.3%), concentration difficulties (24.2%), insomnia (20.5%), depression (19.7%) |
For those who experience Long COVID, a gradual improvement in symptoms may be experienced, but a plateau is common 6-12 months post-infection. Only 22% recover fully within a year.30
We Are All Pre-Disabled
According to recent data from the CDC Household Pulse Survey,31 approximately 18% of USA adults have experienced Long COVID, highlighting the vast scale of this condition, especially when extrapolated worldwide. Long COVID’s economic and societal impacts are already profound and individuals continue to experience symptoms years after their initial infection. Age, pre-infection resilience, and physical capacity—in other words, how one “feels”—are not determinants of vulnerability to Long COVID, and the parts of the body affected are unpredictable. Children,32 marathon runners, and rich celebrities are just as vulnerable to these long-term conditions as everyone else.
Cognitive Impairment
Among the most debilitating aspects of Long COVID is its impact on brain function.33,34,35,36 Cognitive dysfunction—"brain fog"—affects a significant portion of Long COVID patients, with symptoms like memory loss, difficulty concentrating, and impaired decision-making. These impairments can severely disrupt education, careers, and daily life. As detailed above, cognitive issues often persist for years after infection.
Cognitive impairment is one of the most concerning and prevalent consequences of Long COVID, presenting as a neurodegenerative condition similar to Alzheimer's, dementia, Parkinson's, and Chronic Traumatic Encephalopathy.37 This form of cognitive decline is not only debilitating in terms of memory, focus, and decision-making abilities but can profoundly affect one’s ability to function in daily life. Often, affected persons struggle more with cognitive tasks such as attention, visual processing, and processing speed, particularly after brain regions like the cerebellum—essential for motor control and cognition—suffer from atrophy.38 This dysfunction can result in slower cognitive processing, making it harder to think clearly or focus, even long after the infection has passed.
Research has revealed that even mild cases of COVID–19 can cause significant brain damage, especially in areas critical for cognition. Studies show that less than six months after infection some patients lost up to 2% of brain volume, nearly ten times greater than the normal annual loss seen in older adults.39 Loss was observed in specific regions including the part of the brain involved in sensory processing (likely responsible for loss of taste and smell), and the part crucial for memory and spatial processing (likely responsible for symptoms like brain fog, memory loss, and confusion). These findings suggest that Long COVID can cause structural changes in the brain that may lead to lasting cognitive impairments.
Moreover, the impact of COVID on cognitive function is not just immediate. Long-term studies have found that even two years after infection, there is an increased risk of cognitive deficits and dementia, especially when compared to other respiratory infections. This suggests that COVID may accelerate cognitive decline in previously healthy people.
Chronic Fatigue
Severe, unrelenting fatigue is another hallmark of Long COVID. Unlike ordinary tiredness, this exhaustion can be debilitating as rest is not restorative. Long COVID fatigue can render people unable to maintain employment or inhibit their ability to perform basic tasks. Fatigue becomes more prevalent over time, affecting over one-third of Long COVID sufferers after two years.40
Mental Health Challenges
Long COVID is associated with profound effects on mental health, contributing to increased rates of depression and anxiety.41 These conditions not only diminish quality of life but add an additional layer of suffering that complicates recovery from other long-term symptoms.
Cardio-Respiratory and Gastrointestinal Complications
Long COVID frequently manifests as ongoing cardio-respiratory symptoms, such as shortness of breath, chest pain, and heart palpitations, which can significantly impair physical functioning. Additionally, gastrointestinal issues, including abdominal pain and chronic diarrhea, can disrupt nutrition and overall well-being. These symptoms illustrate the systemic nature of Long COVID, which, as a vascular disease, can affect every organ of the body from the lungs and heart to the liver, pancreas, and intestines.42
Immunological Impact
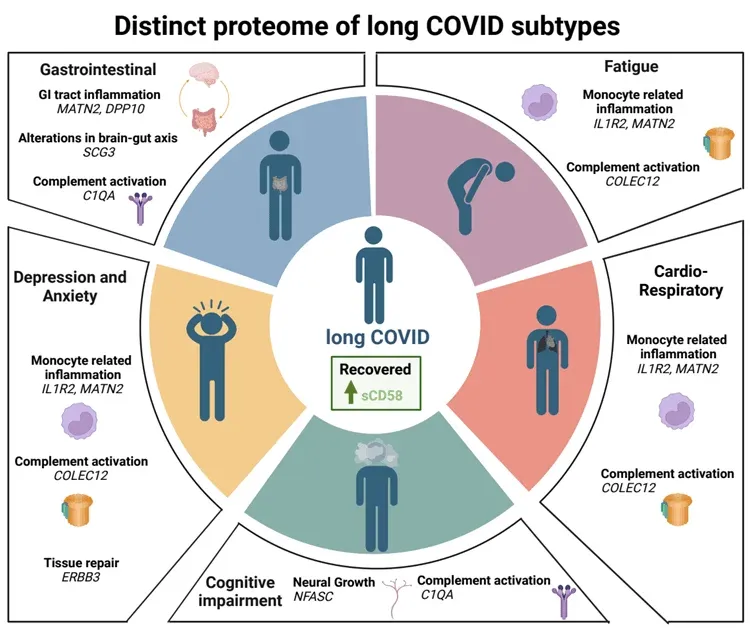
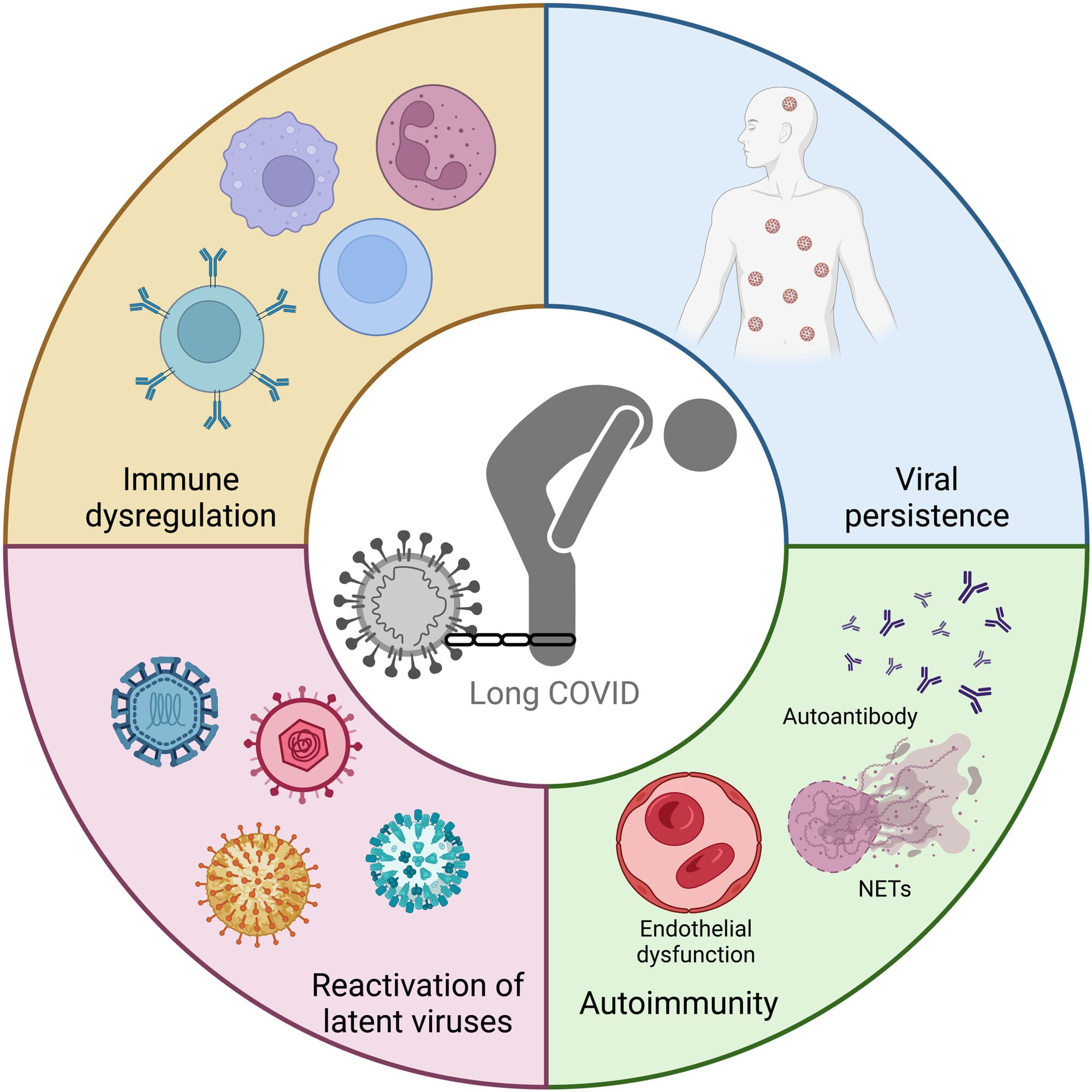
Unidentified in the graphs above was the potential underlying change acute COVID-19 infection may make on individual immune systems. Over the course of a long and logical path, some scientists’ hypotheses43 regarding the immunological impact of COVID-19 has recently been proven correct.44,45,46 Immunological impact has also been implicated in the significant amount of asymptomatic/presymptomatic spread.47 The recent identification of the “superantigen” (a foreign body that super-stimulates the immune system, causing collateral damage) opens the door to exploring immunological consequences of infection and repeat infection, especially as they undergird all presentations of Long COVID.48 COVID–19 has been linked to a marked increase in autoimmune disease as well.49
Vulnerable Populations are at Higher Risk
Certain groups face an elevated risk of developing Long COVID, including individuals with cancer, HIV, or immunodeficiencies, and anyone who has previously had an acute COVID–19 infection.
Cancer patients, particularly women, show higher rates of Long COVID, compounding their vulnerability to infections and further straining their health. People living with HIV are more prone to cardiovascular complications and metabolic dysfunctions linked to Long COVID. Those with immunodeficiencies, such as common variable immunodeficiency (CVID) or autoimmune conditions, also face greater risks due to their compromised immune systems. For these populations, preventing Long COVID is not just important—it is lifesaving.
Prevention is Key
While we have learned much about Long COVID since 2020, it’s clear that we are still scratching the surface. While some key associations have been identified with regard to certain presentations of Long COVID50,51,52,53 there are no approved treatments (and no cure) at this time. One bright note is that two HIV antivirals are being repurposed and trialed to address Long COVID, specifically addressing viral persistence, in the same way an HIV antiviral was repurposed for Paxlovid for acute COVID.54 However, the known risk of Long COVID on a per-infection basis has not meaningfully changed as new COVID variants have emerged, and the overall risk has increased due to the increased data availability concerning recovery,55 reinfection, and the development of Long COVID. Prevention is currently the most reliable way to protect long-term individual and public health and reduce the risks associated with Long COVID.
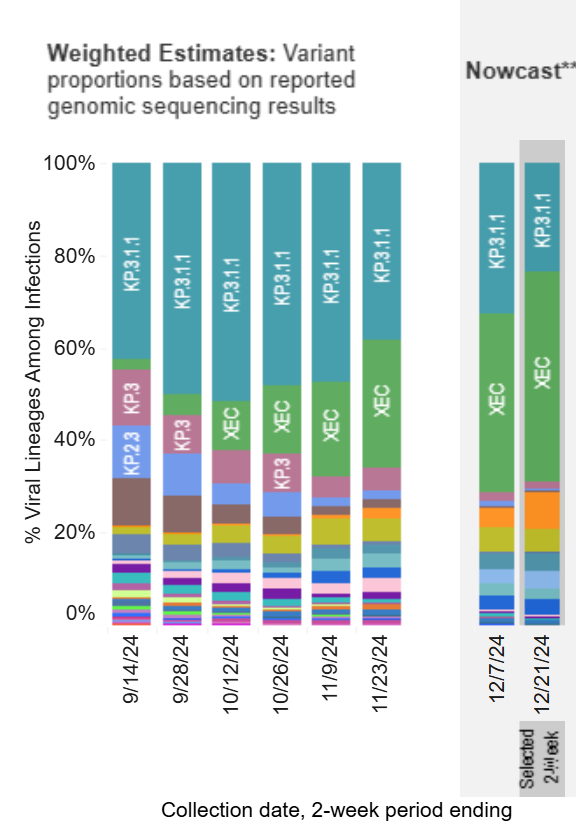
Current Variant(s)
The most prevalent variants this season are still descendants of the JN.1 lineage. Since June, KP.3, KP.2, and LB.1 have been overtaken by KP.3.1.1 and XEC globally and in the continental USA, with XEC en route to dominance.56
What sets KP.3.1.1 and XEC apart are numerous distinct advantages for immune escape,57,58,59,60,61,62,63,64 which reduce the effectiveness of neutralizing antibodies (nAbs) from prior infection or vaccination. Immune escape allows the virus to evade recognition by existing nAbs, reducing the protection of prior immunity. New antibodies can still be generated by new infection or updated vaccination. It increasingly appears SARS-CoV-2 can become persistent (i.e. as one cause of Long COVID),65,66 which in itself is a form of immune escape.
These new variants do not exhibit different symptoms compared to previous ones. For approximately the last 1.5 years, in the XBB/BA2.86/JN.1 era, the most common symptoms have been: fever, chills, cough, shortness of breath or difficulty breathing, fatigue, muscle or body aches, headache, new loss of taste or smell, sore throat, congestion or runny nose, nausea or vomiting, and diarrhea.67,68,69 If you, or anyone with whom you have shared air, develop any of these symptoms, you should consider testing.
Proactive Considerations
Infection Rates
Wastewater and emergency department data suggest that the USA has ended its Autumn wave and is already beginning a Winter wave.70 Cases in England have been flat for the past four weeks, but the risk remains high.71 While cases may be relatively low for the holidays, gatherings will only accelerate spread.
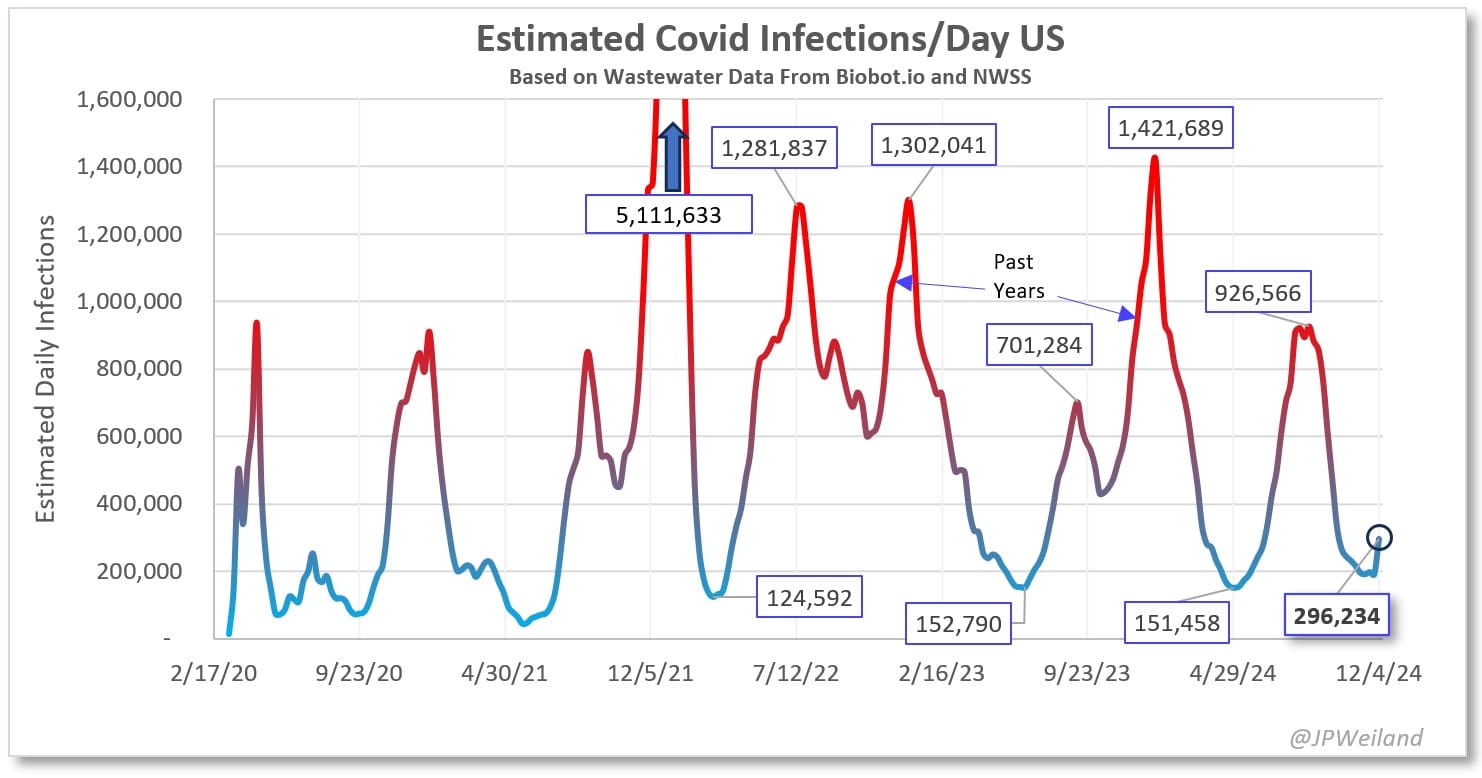
While the same safety measures are recommended regardless of if a wave is occurring or not, it is important to identify just how much danger one is in at any time for the purpose of scheduling necessary dental or medical care that might involve unmasking. Unfortunately, the danger is continuing to increase, since even case counts during troughs are at what should be considered emergency levels (and lower levels were in 2020).
Vaccination
Staying up to date on vaccinations remains an important tool in the toolbox. However, vaccination is not something that can be relied upon singularly for protection. As things stand with currently available COVID–19 vaccines, a vaccination is like an airbag in a vehicle: something you absolutely want to have but never want to put to the test.
The vaccines currently available in the United States since early 2024 remain efficacious against severe acute disease at the time of infection from the period 2–4 weeks after injection up to 4–6 months following injection.72 After 4–6 months, while there is lag time between the infection and the production of antibodies, despite concerns regarding antigenic imprinting, in the acute phase of a COVID infection it does offer a level of protection from current variants (primarily descended from JN.1) against death, critical illness, hospitalization, and symptomatic acute infection. However, it does not do so at a level that justifies abandoning other tools like masking. Similarly, no vaccine offers sufficient protection against Long COVID to justify unmasking.73,74,75
Special Note: Masking And Social-Emotional Development
After significant review of studies on respirator usage and social-emotional development, the previous broad conclusion was that there was a reduction in the capacity of infants, toddlers, and children to identify emotions by approximately 10%; however, a follow-up study76 has clarified that adaptation is rapid within a peer group and this 10% is anticipated to revert to zero with experience and exposure. Moreover, research on populations with long-term face covering (veils, etc.) or sensory differences (e.g. blindness) suggest no significant developmental delays.
Conclusion
New vaccine technology on the horizon currently projects a 2029 target for a shift in our approach to the pandemic. All available information on Long COVID reinforces the importance of ongoing vigilance to safeguard our health and that of our loved ones. The increasing dominance of more infectious and immune-evasive variants underscores the urgency of staying informed.
Unsurprisingly, political challenges will continue. The new U.S. federal administration is nominating a co-author of the eugenic Great Barrington Declaration, Jay Bhattacharya, to head NIH, and the anti-vaccination huckster Robert F. Kennedy Jr. is being given a prominent role. Without community support and care, few have the capacity to face each day’s challenges in this arena. Regularly updated information and the publication of these updates is vital, and represents SCORE’s collective commitment to our ever-expanding community.
Timeless Toolbox
Some items are not seasonal or in response to a known infection, and are instead persistent tools of pandemic self-defense.
Risk of Acute Infection
SARS-CoV-2 is a virus which causes a vascular disease process (COVID) and which is transmitted primarily by a respiratory route. In other words, COVID spreads via one person breathing out and another person breathing that same air in. The majority of transmission occurs before symptoms appear.77,78 Additionally, COVID can hang in the air for over 12 hours,79 meaning that even an empty room is not necessarily a safe room (e.g. an empty exam room in a medical clinic, an empty aisle of a supermarket, or a public toilet). This has not changed as new COVID variants have emerged. Since the SARS-CoV-2 virus travels through and lingers in the air like smoke, indoor spaces have especially high potential for infection. However, it is important to understand that one can also easily be infected outdoors. There is overwhelming, documented evidence of outdoor transmission.80,81,82,83,84
The Relative Infectiousness (relative “Growth Advantage”) of dominant variants has only increased. In other words, risk due to wearing a low-quality mask, or a high-quality mask which is not fit-tested, or not masking outside, has increased. More precaution is needed now than was needed previously to avoid infection.85,86
Even though the SARS-CoV-2 virus can survive for a long time in lab conditions, many studies suggest that it is not likely to spread by touching non-living surfaces on which the virus is deposited (fomite transmission).87,88,89,90,91,92 There is a growing body of evidence that glasses wear lowers the risk of COVID, at least for contact with gross droplets (e.g. being sneezed on); however, the significance remains unknown.93
There is a growing body of evidence for zoonosis (transmission from animals to humans)94 and reverse zoonosis (transmission from humans to animals).95 It is important to keep this in mind, both to keep oneself safe from one’s pets and to keep one’s pets safe from oneself. Cats, dogs, and rats frequently get infected by the virus and suffer from its effects, both in the acute phase and in the long term.96,97,98,99,100
Testing
As part of the Biden administration’s plan to privatize the response to the pandemic, the cost burden of testing has been shifted to the individual. Not only has the government’s free rapid test program been discontinued, but the free drive-thru PCR sites that were so common earlier in the pandemic have been dismantled. For most, getting a PCR test now involves making a doctor’s appointment, paying for the test out of pocket, and, consequently, a high risk of COVID exposure or spreading COVID due to the lack of infection control in medical settings.
The following infographic was posted by Twitter/X account @Clean_Air_Club_ and is shared here with its citations. The original post is available here (at the time of writing) and archived here. Citations include:101,102,103,104,105,106,107 Over the last 4.5 years, the median (not average) time between exposure and the presence of detectable infection (COVID Incubation Period) has reduced from 5 days to 3.75 days.108
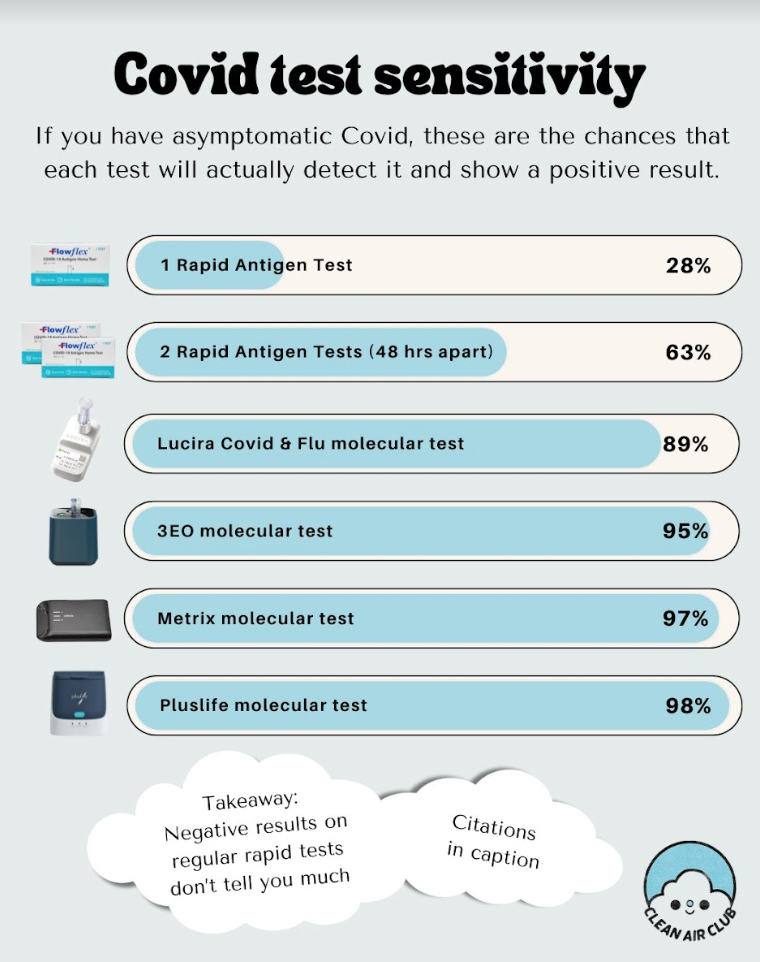
Rapid Antigen Tests (RATs) remain the least expensive but least accurate method of testing for COVID. The following caveats are extremely important for understanding RATs:
- A single positive result on a RAT means you have been infected and are contagious.
- A single negative result on a RAT, however, does not mean you do not have COVID. False negatives on RATs, especially when asymptomatic or presymptomatic, are extremely common, to the order of approximately 72%.109 Even with symptomatic infections, it is common for people to consistently test negative several days after their symptoms begin.
- The FDA recommends serial testing with RATs,110 testing two to three times over the course of three to five days, depending on the brand of test, which will reduce the risk of a false negative.
In order to increase test accuracy, a combined mouth-throat-nose swab should be performed, because combined location swabbing results in detectable virus 1-2 days earlier.111 The nose portion should be carried out by swabbing one’s nasal cavity instead of swabbing up one’s nostrils. This has been established as best practice ever since the original Omicron variant became dominant.112 Please see a nose swab video demonstration here and throat swab instructions here.
There are also a number of much more accurate but more expensive home molecular tests on the market. On top of the increased cost, these have a tendency to error out and unlike RATs can have a non-negligible false positive rate. However, these tests have an 89% to 97% chance of detecting an asymptomatic COVID infection.
The primary new development in testing this season is that there is now a new home molecular test (PlusLife) that not only has a 98% chance of detecting an asymptomatic COVID infection but also has an extremely low false negative and positive rate. Its primary improvement over prior tests in this range of sensitivity is a report of quantitative (graphical) results instead of a “yes / no” result (or “error”). For more information and extensive research, check the excellent community-made FAQ at here.
Prompt Response To Infection
Upon suspecting or confirming you have been infected, it is important to immediately isolate oneself from others so as not to infect them. Despite how transmissible SARS-CoV-2 is, it is possible to avoid in-home transmission through a combination of N95 masks, air purifiers, and ventilation. Some guidelines:
- The infected person should be isolated in a room with a window fan blowing OUT the window, with an air purifier running, and with any gaps in the door stuffed or sealed.
- The non-infected persons will avoid entering that room, run air purifiers, and have window fans blowing fresh air INTO their living space.
- Non-infected person should wear a respirator when they must share air with the infected person, or if they’re caring for the infected person.
- Whenever the infected person has to leave the isolation room (i.e. to go to the bathroom), they should be wearing an N95. Ventilate the bathroom fully or wear an N95 if using the bathroom soon after the infected person has used it.
The more time that all parties can wear an N95, the less of a chance of transmission. More detailed information on how to prevent spread has been compiled by Clean Air Crew here.
Effective Mitigations
Paxlovid
Paxlovid (orally administered Nirmetralvir+Ritonavir) is currently the only antiviral medication proven effective against COVID (excluding Molnupiravir for its questionable efficacy). It inhibits viral replication, thereby reducing acute infection severity, the risk of hospitalization, and the risk of death. Furthermore, it has been proven to reduce one’s chances of developing Long COVID.113,114 If infected, it is vital to take Paxlovid if you are medically able regardless of perceived infection or symptom severity, and ideally as quickly as possible.
Paxlovid is typically issued as a 5 day course. Sometimes symptoms improve over those five days but then begin to return. This situation, often referred to as “Paxlovid rebound,” is not caused by Paxlovid, but instead by the 5 day course not being enough to clear the virus.115,116 A helpful analogy for “Paxlovid rebound” is stopping one’s antibiotic treatment at the sign of improved symptoms but before the infection is overcome. Paxlovid was originally intended to be taken as a 10 day course and is more effective that way,117 and this is in fact the course that Dr. Fauci took when he was first infected.118
Unfortunately, it is not always easy to get a Paxlovid prescription in a timely manner (or at all). Many doctors caution patients that it is only beneficial in especially severe cases or in particularly at-risk populations, or that it causes rebounds or is not effective at all. Unfortunately, a doctor is very important to consult depending on the medications you take that may have harmful interactions with Paxlovid. If one’s doctor refuses to prescribe Paxlovid for an invalid reason (valid reasons being medications or conditions that are dangerous with Paxlovid), a prescription may be obtained through a telehealth service. Some states have their own Paxlovid telehealth lines, and there are several online private telehealth services as well, including Sesame Health, Dr. B, Push Health, and Plush Care.
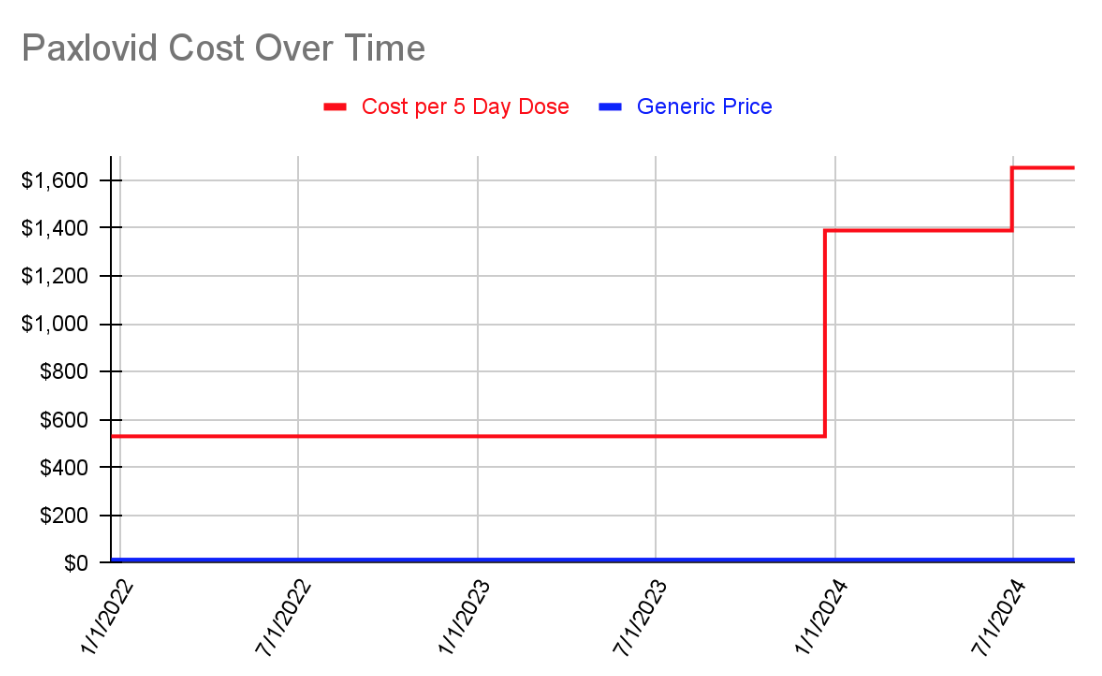
Prior to December 2023, the cost of Paxlovid was covered entirely by the US government. The cost has since been shifted to the individual and dramatically increased. The estimated generic cost of a 5 day course of Paxlovid is $15.08.119 For the duration of time it was covered by the government, the price was set at $530.120 When the government stopped covering it, the price increased to $1390121 and then again to $1692 before insurance.122
Rest
Rest is absolutely essential after being infected—too much physical activity while infected or before one’s body has fully recovered increases the chances of developing Long COVID. This is a serious vascular disease that can damage every system in one’s body invisibly. At the very least, it is recommended to wait seven to ten days after being symptom free and testing negative before returning to exercise, but the more rest the better—three months is ideal.123124 When finally trying to exercise again, it is important to do so very minimally and gradually, and stop immediately at the sign of any limitations, issues, or unnatural fatigue. A heart-rate monitor should be worn as well.125
Metformin
Metformin—a common, inexpensive diabetes medication—may reduce one’s chances of developing Long COVID after infection. A promising study from earlier in the pandemic showed a 40% reduction in Long COVID, 126 and a new study has just been released showing a 42% reduction in Long COVID, a 3.6x reduction in viral load by day ten, a 58% reduction in the risk of hospitalization, and a 32% reduction in the risk of rebound.127 It is something worth discussing with one’s doctor.
K12 Oral Probiotics
There is evidence that, once one tests positive, taking Streptococcus Salivarius K12 Oral Probiotics for at least two weeks can reduce the severity of one’s COVID infection.128 These probiotics are available without a prescription and can be found online and at pharmacies. They do not have a prophylactic effect (they do not prevent infection or protect against infection).
Nasal Irrigation
On top of being a tool to use pre-exposure, nasal irrigation can be used post-exposure in order to help relieve symptoms and help one’s body clear the virus faster.
There is evidence that rinsing one’s nasal passages after a potential exposure can help prevent the virus from taking hold or possibly reduce the viral load one’s system is exposed to (and thereby possibly reduce the length and severity of illness).129 One will need distilled or boiled water, saline packets, and either a neti pot or a squeeze bottle. More information including a detailed walkthrough has been shared by Clean Air Club on Twitter/X here, archived here.
Studies have shown (references indicated below) that over-the-counter Iota-Carrageenan,130,131,132,133,134,135 Hypromellose,136 Nitric Oxide,137 and Xylitol 138 nasal sprays can reduce one’s chances of developing a COVID infection if exposed. Overall, though, the evidence can be summarized to say that doing some kind of nasal irrigation will result in some amount of risk reduction.
In general, these sprays can be used both before and after a potential exposure. It is important to understand that these sprays are not a replacement for wearing a respirator and that the listed protection percentages are potential reductions in risk—nasal sprays should be viewed as a merely extra layer of protection, and one that is potentially useful for situations where unmasking is required (dental care, certain medical procedures, etc.). Discussion of the studies and results above has been shared on Twitter/X by Clean Air Club here, archived here.
Respirators
Wearing a respirator that fits you (whether a disposable N95 or an elastomeric with P100 filters) remains the single most effective way of protecting oneself from getting infected and infecting others. A P100 or N100 offers protection against COVID measured at >99.97%.139
The best respirator is a respirator that fits you. In order to truly know if one’s respirator fits properly, a fit test must be performed. A fit test involves wearing a respirator, placing a hood over one’s head, spraying a fit test solution (e.g. Bitrex or its sweet counterpart), and attempting to taste it while performing a set of motions.140 This can be accomplished inexpensively at home by using a face mister and a garbage bag. If you cannot taste the solution, that means your respirator fits you properly. If you can taste the solution, that means your respirator either is not positioned correctly on your face and needs adjusting, or that it does not fit you and a different model is required.
For disposable respirators, the 3M 9210+ Aura is a trusted respirator that is likely to fit most faces. If the Aura feels too small, the 3M 9105 Vflex or Dräger 1950 are good options. If the Aura feels too large or if you are trying to find an N95 that fits children, the Trident P2 respirator may be a good fit.
For elastomerics, the 3M 7500 series (with 7093 P100 filters) and the 3M HF-800 Secure Click series (with D9093 P100) filters are excellent choices. The Flo Mask can be a great option for children ages 4 to 12 as well although many substitute the filter media.
Mask Bans
Throughout the world, anti-masking laws are starting to gain traction, while the lifting of pandemic emergency orders is by consequence reapplying existing, racist, anti-face covering laws. These bans are a response to increasing pressure from the people for Palestinian liberation, redress for inequality and police brutality, and disability justice. The severity, speed, and spread of the response shows us how threatening our movements are to capital. Politicians will exploit ongoing conflict to undermine and stigmatize masking, and it only hurts us all.141 Further details and potential actions for self-defense and solidarity will be explored in a future update.
For people living in areas with anti-mask legislation, it is recommended to obtain a doctor’s note that explains one’s respirator is being worn for medical purposes and to keep it on one’s person.
Air Filtering / Air Cleaning
Air filters, both store-bought HEPA filters and homemade Corsi-Rosenthal Boxes (commonly referred to as Corsi Cubes), remain important and variant-proof tools in the fight against COVID. SARS-CoV-2 is airborne, and these devices remove the virus from the air.
If you decide to buy a HEPA air filter, choose one that has an appropriate CADR (Clean Air Delivery Rate) while also factoring in other variables like cost and noise. CADR is reported in cubic feet of air filtered per minute. The higher the CADR, the faster the purifier can remove viruses from the air.
An appropriate CADR can be determined mathematically based on the size of the closed-off location you want to keep safe. Here is a link to one of many freely available ACH calculators to help with sizing. Due to the efficiency of air filters, it is always good to add a safety factor of 63% to the final result.
Consider a bare minimum ACH of 4, a reasonable minimum target of 6, and an ideal target 12 (or higher) for protecting oneself from being present with someone with an active COVID infection. Note that air filters, which require multiple passes to clean air, will not be able to reliably prevent a physically present infectious person from infecting you so should not be understood as a way to safely remove one’s respirator indoors with someone else. Air filters are valuable for clearing a space that an infected (or possibly infected) person has been in, but now needs to be safe again or as one layer of mitigation in a location requiring vigilance (home with an infected cohabitant; a hotel room; etc.).
A Corsi-Rosenthal Box (also called a CR Box or Corsi Cube) can be an inexpensive alternative to buying a HEPA air filter. It is a type of air filter that can be made easily at home using a box fan, furnace filters rated MERV-13 or better, cardboard, and duct tape. Despite not using HEPA-rated filters, these filters can outperform many HEPA filters due to their capability to move large volumes of air quickly.
More information, including a comparison of various HEPA air filters and detailed instructions for assembling a Corsi Cube, can be found here.
Finally, when simply ventilating a space rather than cleaning it, a CO2 monitor may be beneficial for identifying when that space has been refreshed (when it reaches ambient CO2 levels).
Ultraviolet Light
Conceptually, ultraviolet sanitizers function like air filters, removing pathogens from the air. In the same way as an air purifier, this is a useful additional mitigation for making indoor spaces safe after potential exposure to the virus. At a population level, this tool would reduce spread significantly. However, no air cleaning technology will deactivate or remove the pathogen in the air in the time and space between you and a nearby individual having a conversation before you can breathe it.
The same as with air purifiers, UV will not be able to reliably prevent a physically present infectious person from infecting you so should not be understood as a way to safely remove one’s respirator indoors with someone else. The most reliable and most cost effective protection is a properly worn and fitted respirator.
There are also business interests operating in this space unscrupulously. People should be very wary of ultraviolet sanitizing lights unless they can personally analyze the spectrum and energy level each light emits. Incorrectly manufactured, advertised, purchased, and/or deployed lights can create hazardous ozone, damage skin and eyes, or simply do nothing to keep you safe.
Due to its higher complexity, significant cost, and limited benefit relative to other readily-available tools, it is recommended that many other layers of mitigation are maximized before training to understand and then implementing ultraviolet sanitizers as part of one’s pandemic self-defense.
Wastewater
Wastewater data is the most time-sensitive gauge of COVID transmission and is the most accurate monitoring method, though it is dependent on calibration. As illustrated by this chart from Santa Clara County Public Health, wastewater data reveals cases missed by testing.
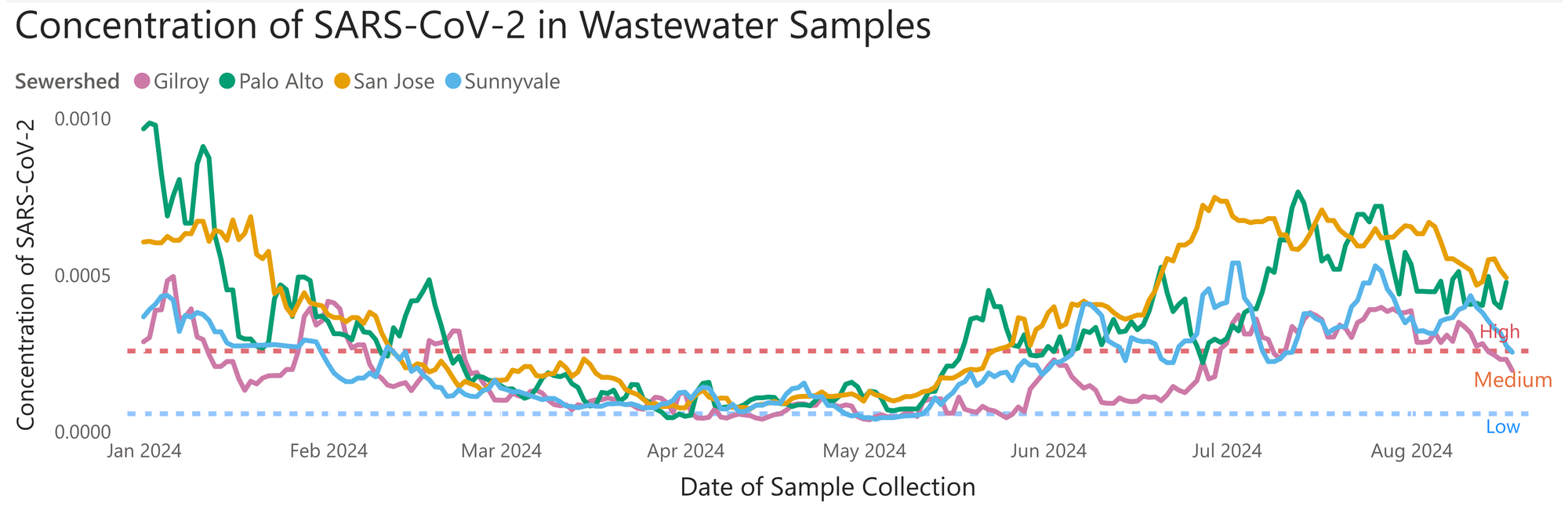
Our capacity to test for COVID at the population level continues to be dismantled. In the USA, the shift from PCR testing to unreported home rapid tests has concealed many infections, with few states having any mechanism for reporting personal RAT results. Having accurate wastewater data has only become more vital. Unfortunately, as pandemic and public health resources continue to be cut, it is becoming more difficult for the average person to find that information. Certain collection sites have unexpectedly stopped reporting data (often with no warning), and the CDC’s decision to end its contract with wastewater surveillance company Biobot to pursue a cheaper contract with Verily has cut the number of wastewater sites it tracks in half (from 400 to 200) and has left 10 states without any information at all.142 For now, we recommend the models produced by the Pandemic Mitigation Collaborative and JPWeiland.
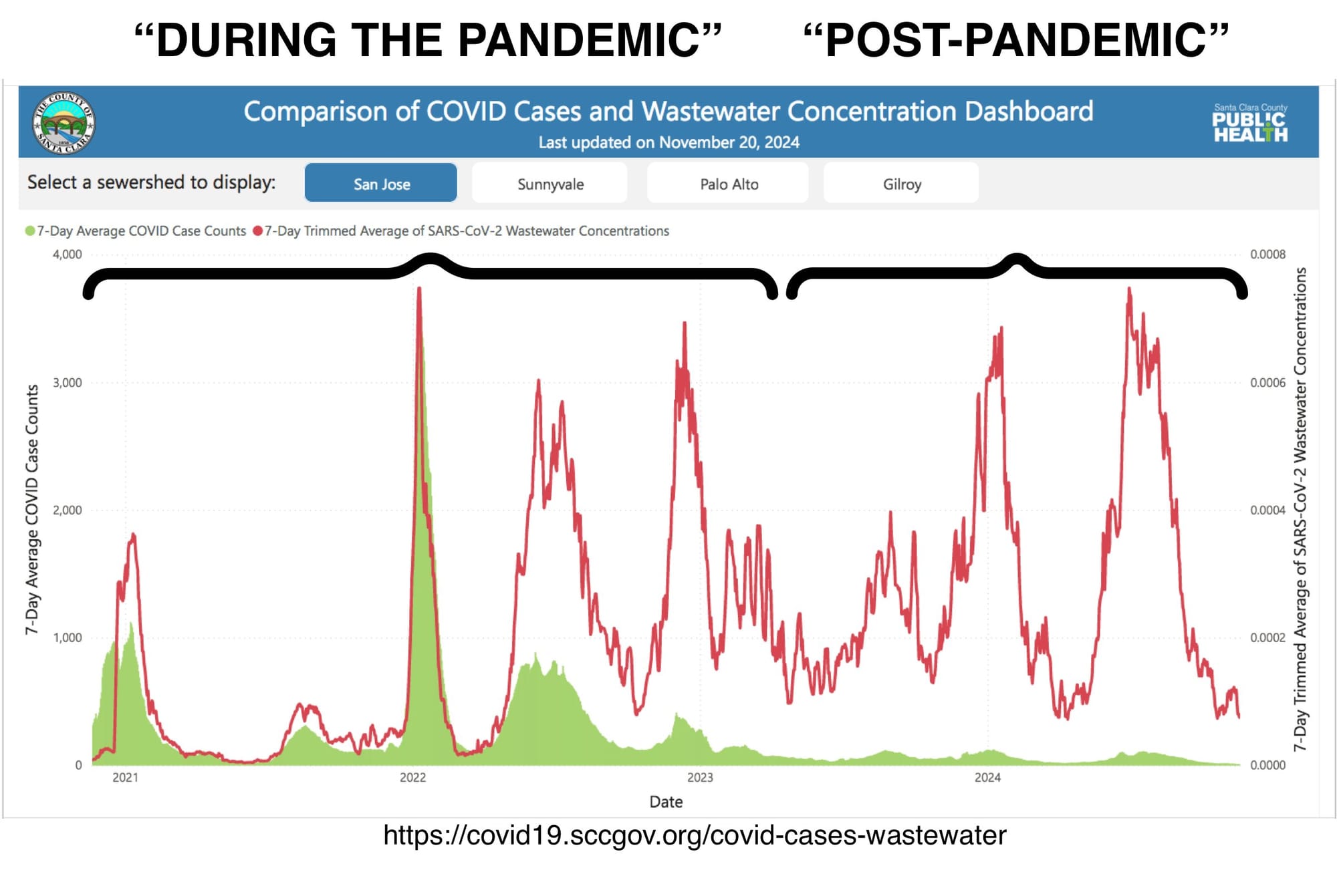
Wastewater data also illuminates the sociological production of the “end” of the pandemic. Consider Lee Altenberg’s fantastic comparison of “During” and “Post-Pandemic” wastewater levels.143
Travel Safety
While it is not recommended to travel during this ongoing pandemic, many people unfortunately are forced to do so by their employers or family obligations. Dynamic Zero will soon publish a COVID Safe Travel Tips article, so please check back with us!